Interpretation of Global Asthma Management and Prevention Strategy Update in 2022 Edition
Correspondent: Sun Yongchang, professor, chief physician.
SETTING: Department of Respiratory and Critical Care Medicine
A cross-sectional study of the first phase of the global asthma network published by The Lancet shows that by providing effective asthma treatment, the heavy burden of severe asthma symptoms in the world can be reduced. However, the prevalence of asthma in China is increasing year by year, and the overall control level of asthma in China is still not ideal. On World Asthma Day in 2022, global initiative for asthma Expert Group released the 2022 edition of Global Asthma Management and Prevention Strategy (GINA 2022). As an important guide for global asthma prevention and control, what are the important revisions of GINA 2022?
Based on this, this paper interprets the update points of GINA 2022, discusses the management of asthma during COVID-19 epidemic, and puts forward the reference significance for the diagnosis and treatment of asthma in China.
01、The diagnostic procedure of asthma was revised.
1.GINA 2022 pointed out that the examination method needed for diagnosis depends on whether the patient has received controlled treatment or not, and explained the matters needing attention during examination, as shown in Figure 1.
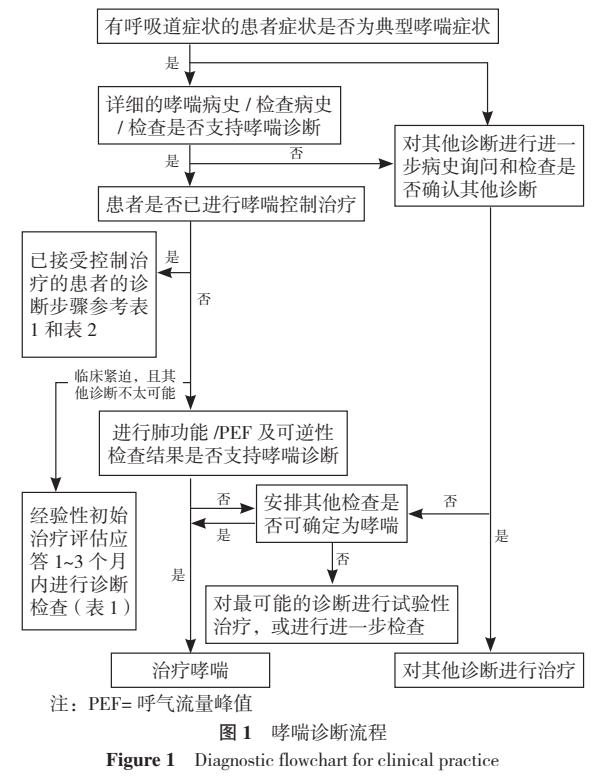
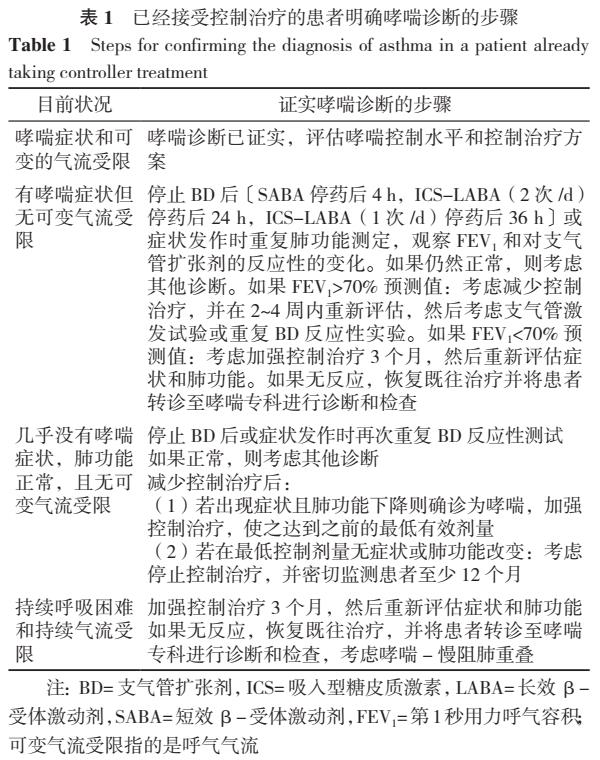
2、For patients who have not received controlled treatment, evidence helpful for asthma diagnosis should be recorded when asthma symptoms appear for the first time; For patients who have received controlled treatment, if the diagnosis basis of asthma has not been recorded before, they should be diagnosed through objective tests, as shown in Table 1.
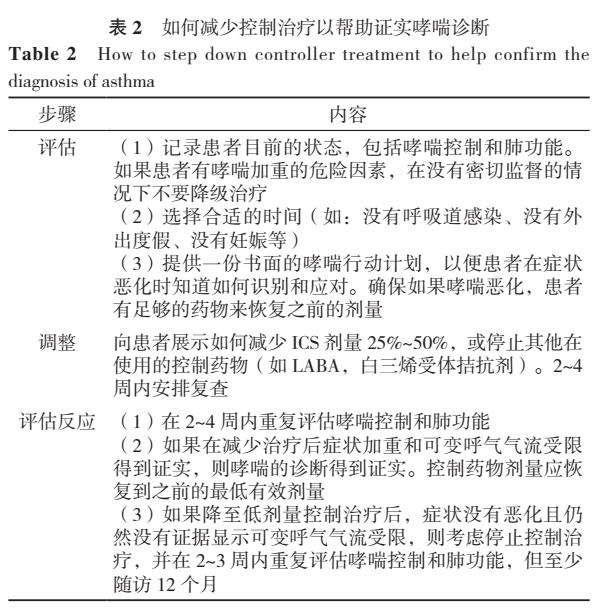
How to reduce the control treatment to help confirm the diagnosis process of asthma is shown in Table 2.
02、Diagnosis and treatment of asthma in low-and middle-income countriesThe treatment plan provides suggestions.
1.GINA 2022 provides detailed guidance on the diagnosis and management of asthma in resource-poor areas. Among them, differential diagnosis usually needs to include endemic respiratory diseases and infections, tuberculosis and human immunodeficiency virus (HIV)/ AIDS.
2.GINA 2022 does not recommend diagnosis only based on clinical symptoms. When the pulmonary function cannot be measured, the peak expiratory flow (PEF) can be used to confirm that the variable expiratory flow is limited.
3.The World Health Organization (WHO) basic non-communicable diseases (PEN) intervention package lists PEF detection as a basic tool for managing chronic respiratory diseases, and WHO-PEN suggests that compared with COPD and other diagnoses, the improvement of PEF by ≥20% after inhaling 2 sprays of salbutamol for 15 minutes can increase the possibility of asthma diagnosis.
4.GINA 2022 also suggested that after 4 weeks of anti-inflammatory experimental treatment and 1 week of oral glucocorticoid (OCS) treatment if necessary, if the symptoms and PEF are improved, it will help to diagnose asthma (or prompt other diagnosis) before starting long-term controlled treatment.
03、On-demand inhaled glucocorticoids (ICS)- formoterolThe role of frequency of use in asthma control evaluation
ICS- formoterol as a remission agent, its frequency of use (≤2 times/week or > 2 times/week) is not included in the comprehensive evaluation of symptom control. However, the average frequency of using ICS- formoterol on demand should still be considered in the treatment decision.
04、Opinions on the severity of disease and "mild asthma"
GINA 2022 suggested that the word "mild asthma" should be avoided as much as possible in clinical practice; If it is used, the risk of serious attack and the necessity of using ICS-containing treatment scheme should be reminded.
05、Treatment of asthma
In the maintenance treatment of asthma, some issues are still controversial, such as the use of long-acting anticholinergic drugs (LAMA), whether to add some new biological targeted drugs to the fifth grade treatment of asthma, etc. GINA 2022 recommended the above problems and provided evidence. See figure 2.
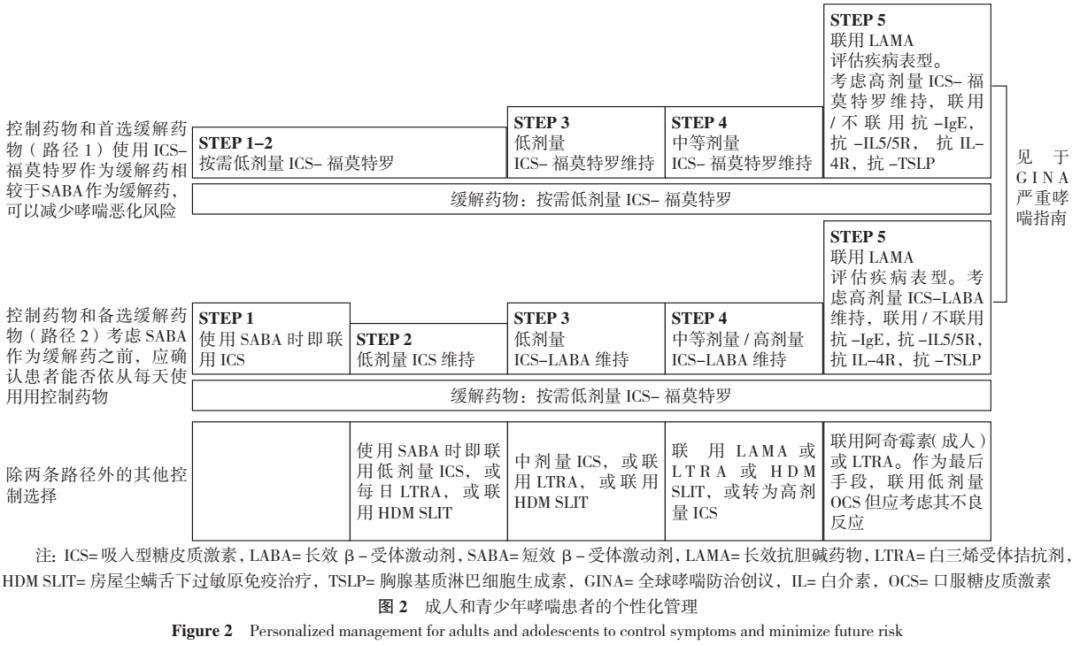
Specific to the treatment of asthma in adults and adolescents, GINA 2022 emphasizes the reasons for two treatment paths:
Path 1, ICS- formoterol is used as a remission agent as needed in the treatment process because it has lower risk of acute attack and similar symptom control effect compared with SABA as a remission agent.
Path 2, GINA 2022 also added other evidence for the low-dose on-demand use of ICS- formoterol in step 1-2, including systematic review showing that the on-demand use of ICS- formoterol significantly reduced the risk of emergency treatment or hospitalization compared with daily ICS combined with on-demand SABA. GINA 2022 included anti-TSLP as a new biotherapy for severe asthma in step 5, and introduced it in detail in the guide to severe asthma.
06、Decision Tree of Refractory and Severe Asthma in Adults and Adolescents
(1)GINA 2022 clearly points out that for patients with refractory asthma whose blood eosinophils are ≥300 /μl, before considering biotherapy, we should evaluate whether there are any non-asthmatic causes, including strongyloides infection (strongyloides infection is usually asymptomatic). For patients with eosinophilia (blood eosinophils ≥1 500 /μl), eosinophilic granuloma with polyangiitis (EGPA) and other reasons should be considered, and the use of anti-IL4R should be avoided, because such patients were not included in the phase III study.
(2)GINA 2022 decision tree mentioned that tezepelumab is an additional biotherapy for severe asthma patients over 12 years old, and it has the greatest benefit in reducing the risk of acute exacerbation for patients with hypereosinophilia or screaming out nitric oxide (FeNO).
(3)Anti-IL4R is added for adults and teenagers.
(4)Anti-IgE is added during pregnancy, and there is very little evidence about the treatment of severe asthma during pregnancy, and the risk of using biotherapy during pregnancy needs to be weighed against the risk of uncontrolled asthma to mother and baby. A registered study found that using omalizumab during pregnancy did not increase the risk of congenital malformation.
(5)GINA 2022 added the results of systematic review and meta-analysis of patients with eosinophilia and type 2 asthma with additional application of anti-IgE, anti-IL5/5R and anti-IL4R.
(6)Maintenance OCS is only used as the last treatment for all age groups when other treatments are ineffective and there is no alternative.
(Note: You can swipe up and down to see more)
07、Asthma-chronic obstructive pulmonary disease (ACO)
(1) Definition: ACO and asthma+chronic obstructive pulmonary disease (COPD) are used to collectively refer to patients with persistent airflow limitation with clinical characteristics of both asthma and COPD. This is not a definition of a single disease, but is used to describe some clinical phenotypes with different pathogenesis.
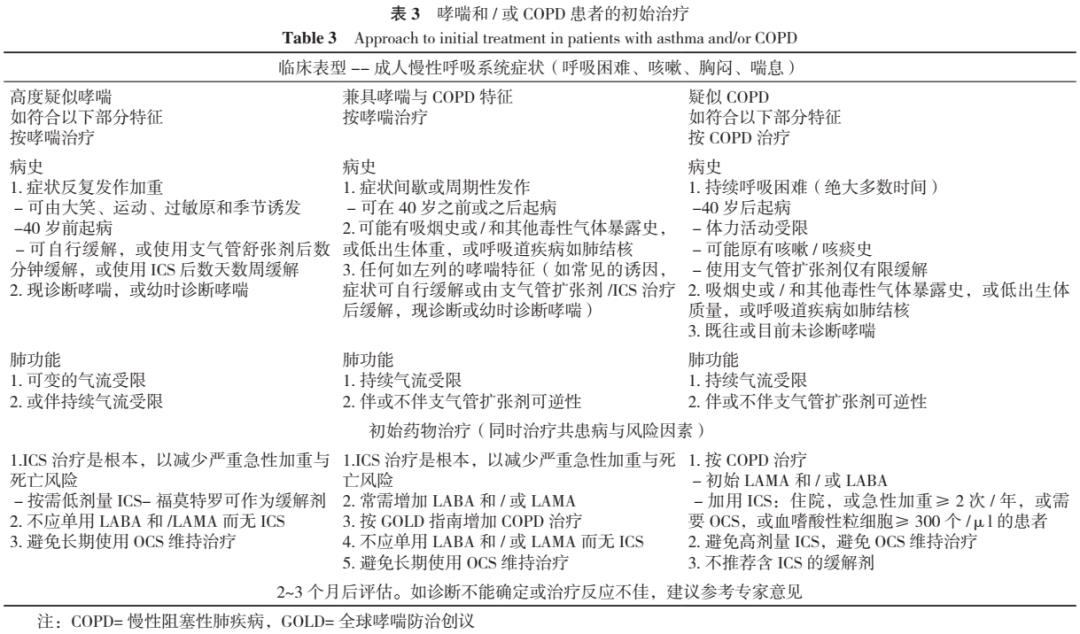
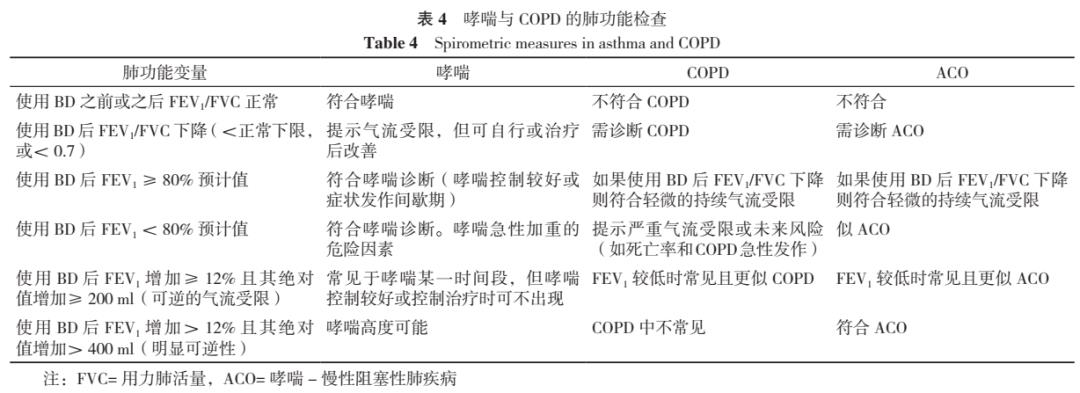
(2) Diagnosis: See Table 3 for the most helpful clinical features and corresponding recommended treatments to distinguish asthma from COPD, and Table 4 for the pulmonary function features of ACO.
(3) Treatment: initial treatment (see Table 3), ACO should be treated as asthma, and ICS is the key to treatment.
Referral examination, it is recommended to refer for further diagnosis and evaluation in the following cases:
① Patients with persistent and/or worsening symptoms after treatment;
② The diagnosis is uncertain, especially the need for further differential diagnosis, such as bronchiectasis, post-tuberculosis scar, bronchiolitis, pulmonary fibrosis, pulmonary hypertension, cardiovascular diseases and other diseases that cause respiratory symptoms;
③ Suspected asthma or COPD with atypical symptoms or other symptoms and signs (such as hemoptysis, obvious emaciation, night sweats, fever, bronchiectasis or other structural lung diseases) should be referred as soon as possible without waiting for the treatment trial of asthma or COPD;
④ When chronic airway diseases are suspected, but the characteristics of ACO are few;
⑤ Complications of patients may affect the assessment and management of respiratory diseases;
⑥ According to GINA and GOLD, problems during the treatment and management of asthma, COPD or ACO should also be referred.
08、Other update points
(1) Using electronic cigarettes will increase the risk of respiratory symptoms and acute exacerbation of asthma;
(2) Air filter can reduce the exposure of fine particles, but there is no consistent result for the prognosis of asthma;
(3) Updated the evidence of correlation between air pollution and the utilization of emergency medical care resources for asthma;
(4) Electronic inhaler detection can identify the compliance of patients with refractory asthma;
(5) In the patients who have used the treatment scheme containing moderate-high dose ICS, but the asthma symptoms are still not controlled, high blood eosinophil level and high FeNO level are related to the high risk of acute exacerbation of asthma;
(6) Patients hospitalized due to acute asthma attack should continue or be given a treatment plan containing ICS.
Management of asthma during COVID-19 epidemic
1. Management of asthma during 1.COVID-19 epidemic.
GINA 2022 pointed out that asthma patients did not seem to have an increased risk of COVID-19 infection. However, it should be noted that the risk of death caused by COVID-19 increases in patients who need OCS for asthma and hospitalized patients with severe asthma. It shows that it is very important to continue good asthma management, and active measures should be taken to maintain good symptom control, reduce the risk of acute exacerbation of asthma and minimize the demand for OCS.
2. The requirements of epidemic prevention and control should be considered in the process of asthma management.
If it is impossible to test lung function due to the restriction of local epidemic prevention and control, and the information about lung function is needed, we can consider asking patients to test lung function at home. Some treatment measures, such as oxygen therapy, sputum induction, manual ventilation, non-invasive ventilation and intubation, can lead to the generation of aerosol, so we should follow the local health strategies and health suggestions on the use of personal protective equipment in accordance with the requirements of epidemic prevention and control.
3. Suggestions on vaccination of asthma patients with COVID-19 vaccine.
(1)GINA suggested that patients with asthma should be vaccinated with COVID-19 vaccine in time and booster if possible. At the time of vaccination, the usual vaccine preventive measures are also applicable to asthma patients.
(2) For patients undergoing biotherapy, the first dose of biotherapy and COVID-19 vaccine should not be injected on the same day, so as to identify their adverse reactions more easily.
(3)GINA also reminded that asthma patients should be vaccinated with influenza vaccine every year, and influenza vaccine and COVID-19 vaccine can be vaccinated on the same day. In addition, even if vaccinated, you should wear a mask in public places.
Reference significance for asthma management in China
1.For the diagnosis of asthma in China, we should pay attention to the following points.
(1) It should be emphasized in medical institutions at all levels that the diagnosis of asthma should be based on the objective basis of symptoms and signs and variable airflow limitation.
(2) When the first symptoms appear, whether to carry out further examination should be decided according to its clinical urgency. If necessary, the lung function data or variable airflow limitation data should be recorded. For patients who have received treatment but have no asthma-related data records, relevant examinations should be improved according to their control situation.
2.In the evaluation of asthma control, use "mild asthma" cautiously.
The term "mild asthma" should be avoided in clinical practice. If necessary, patients with infrequent symptoms or mild asthma symptoms may still have severe or fatal attacks, and this risk can be reduced by half or even two-thirds by using low-dose ICS or low-dose ICS- formoterol as needed.
3.About the treatment and management of asthma
(1) Attention should be paid to individualization of treatment, and the treatment decision should take into account the characteristics or phenotypes of patients, which may predict the difference of treatment response between them and other asthma patients. In addition, the patient’s expectation of therapeutic effect, psychological burden and some practical problems (inhaler technology, compliance, ability to use drugs, patient’s cost, etc.) should also be considered.
(2) It should be emphasized that low-dose ICS- formoterol as a remission agent is the first choice for most people.
– END –
关于作者